|
Picture yourself on a mountaintop. The piercing cold temperature. The unbarred views. The thin air.
Dr Hugh Montgomery presented the mountaintop to us as a natural laboratory space. As Director of UCL Institute for Human Health and Performance, and Professor of Intensive Care Medicine, Hugh is interested in how the human body responds to exercise. And the mountaintop presents an extreme environment for a particularly elite class of exercisers, the mountaineers. Not only is mountain climbing a gruelling challenge for the body's muscles, but climbers must also tolerate low levels of oxygen in the air. The higher they climb, the lower the oxygen levels fall. But by studying the physical changes that mountain climbers undergo on a climb, and scrutinising the underlying genetic causes, Hugh's research group have produced some startling lessons for critical care of hospital patients. Hugh, smiling and fresh-faced, took to the stand at Bristol M-Shed to discuss his research. He is the kind of researcher who deserves his own HBO television show. This hypothetical show would incorporate genuine scientific research, as well as offering plenty of scope for macho posturing and man vs. death escapades on the mountaintop. Indeed, the man's achievements and hobbies would make any fiction unnecessary. A diver, a record-breaking underwater piano player, an 'occasional' ultra-runner, a mountaineer, author, screenwriter, and a pioneering cardiovascular geneticist. I could easily add more, but I am already lost in awe. "Studying acute physiology can tell you really important things about yourself, and patients," said Hugh. He began by outlining the key scientific tools that we needed to understand. Angiotensin is an important hormone for your blood system, and the renin-angiotensin system (RAS) controls the blood pressure of the body. It is a network of different hormones, including angiotensin, which tweak the size of blood vessels and the amount of water kept in the blood. A key controlling element is angiotensin-converting-enzyme (ACE). A high level of ACE in your RAS raises your blood pressure. "That's where it stopped when I was in medical school," said Hugh. "But it turns out, like most things I was taught at medical school, that wasn't half the story. Because these systems are everywhere - in plants, in locusts, in fish, in jellyfish- all things that have been there for millions of years. And jellyfish don't even have blood pressure!" So RAS and ACE must affect more than blood pressure. In fact, they are found in a huge range of human bodily tissues, from your brain to your eyeballs to your skin. It is now understood that ACE also influences cell growth, inflammation, and metabolism in body tissues, even if the finer details of how it does this are still being uncovered. In the 1980s, it was observed that increased amounts of ACE in rats leads them to develop bigger hearts. Knockout the ACE gene, and hearts can't grow in size. In humans, the old romantic maxim is untrue. Having a big heart is not a good thing - unless your heart has become big due to regular exercise. Otherwise, a large heart is associated with a higher likelihood of heart attack. So whatever causes the increase in size also damages the heart tissues. Based on the studies of ACE and heart size in animals, Hugh needed to see if the link between ACE levels and heart size applied in humans. His group had found two different ACE gene variants - the I allele, and the D allele. People with the I allele produced lower amounts of ACE. People with the D allele produced more ACE. And because everyone has two copies of each gene, any human could have II, ID, or DD. But based on rules of inheritance, in a group of people 25% will have II, 50% will have ID, and the final 25% will have DD. So if Hugh could take a group of humans, measure the differences in their heart size, and then correlate the heart size to the different genes, he would be able to prove ACE was affecting heart size in humans. But how could this be done, and more so, done ethically? There could be many confounding factors affecting heart size. Hugh found the perfect experimental subjects in the form of military recruits. Military recruits all undergo the same strict regime of training and diet. Exercise naturally causes heart growth. So at the end of 8 weeks of training, Hugh would be able to measure differences in heart size, and link this to the I or D alleles. After 8 weeks of training, the recruits with II alleles - producing the lowest levels of ACE - showed heart growth of approximately 2%. In DD recruits, who produced the highest levels of ACE, the heart growth was 6%. Hugh sketched out the scientific reason that ACE caused heart growth. In the RAS system, ACE breaks down kinins, proteins which are involved in blood vessel dilation. High ACE equals low levels of kinin, which means greater growth in heart size. As in most science, the chain of cause and effect was becoming a little long, but we were still with him. So the military recruits proved the link between ACE and heart size. And there was more. Through a muscle fatigue test- a fancy way of saying, how long could each recruit hold a weight at arm's length without buckling - it was proved that II recruits have the best response to exercise. ID recruits respond moderately to exercise, showing only small improvement in muscle fatigue after training. DD, statistically speaking, showed no better improvement by end of their training. Now, back to the mountains. Mountain climbers with II are more likely to reach the peaks than DDs. Similar trends can be seen in other oxygen-hungry sports, like marathon running, where runners are much more likely to have II alleles. Hugh revealed another interesting tidbit. Although gruelling endurance challenges like the Tour de France are dogged by doping scandals, where athletes use erythropoietin hormone to increase red blood cell loads, the ability to accumulate more oxygen on a mountaintop is not actually helpful to your body. To put it more simply- if you put a Tibetan and a Westerner on a mountaintop, the Tibetan's body will generate less haemoglobin. The genetic selection for successful living at high altitudes appears to be in keeping haemoglobin lower. Hugh explained that I or D alleles affect how efficiently mitochondria use oxygen. Mitochondria are the power plants of the cell, generating ATP energy from oxygen. Low ACE levels make mitochondria better at generating ATP from oxygen, even low levels of oxygen. D alleles are more like "leaky batteries" - they lead to a higher level of ACE in the body, which raises oxygen demand. "So what genetics is telling us, is that when oxygen availability is low, we should try to increase the efficiency in which we use the oxygen," commented Hugh. He recalled that the convention treatments for ICU patients in hospital is to try, forcibly, to put oxygen into their bodies. But modern treatment needs to change, as studies have shown forcible oxygen transfusions can increase mortality. Based on lessons from mountaineers, new modes of treatment are being introduced into hospitals to allow oxygen levels to reach lower levels than conventional treatment had allowed. A normal person has an oxygen tension of 12 kPA. On a ward, lower levels of 8 kPa is now being allowed. A level of 6 kPA is still considered very worrisome. However one experienced mountaineer has been able to reach 2 kPA. This is conventionally considered terminal... but for him, it was not. His body was attuned to that low level of oxygen. Many animals adjust their body systems to withstand low oxygen environments. These include a few fish with coincidentally interesting names - the epaulettes shark, the oscar fish, and the Crucian carp - who shut off unnecessary body functions when oxygen levels decline. With a wry grin, Hugh admitted that when he explained his research to his 6-year old son, he was told his research was "very obvious". When a car is low on fuel, you don't leave all its systems running, you tune down to the bare essentials. Why had it taken his father 20 years to work out that the human body does the same? But the most startling and sobering impact of ACE was yet to come. Hugh showed us the relationship between the ACE gene variants and medical conditions, especially in the ICU. In premature babies with under-developed lungs, high ACE levels are associated with respiratory distress. In patients who undergo bypass surgery, II patients with low ACE show better survival rates. In meningitis patients, having the DD alleles is associated with the most severe examples of sudden meningococcal sepsis. It was sobering to realise that survival, especially in the face of respiratory complications, could be so clearly linked to the ACE gene. "In this audience, if we all came down with Adult Respiratory Distress Syndrome and ended up in Bristol ICU, the IIs could have a 90% chance of surviving. Whereas DDs have an over 55% chance of dying. That puts my job in perspective. We like to congratulate ourselves as how good we are when someone lives - but a lot of that living and dying, is down to our genes." Hugh moved onto another lesson of mountaineering - starvation. Hypoxia, meaning low levels of oxygen, causes weight loss. Mountaineers lose both fat and muscle in the hypoxic conditions of the mountain. ICU patients, whose body tissues are low in oxygen, also show weight loss. A key clue is that muscle is lost, along with fat, even in highly active and well-fed mountaineers. A group of Hugh's mountaineers who scaled Everest lost 9 kg each, on average. Hugh explained that the 90% of the body's energy goes into producing protein, to rebuild and renew the body. It used to be thought that in low oxygen conditions, the body's regulation was simply thrown into disarray, causing inevitable weight loss. But now it is shown that the body actually orchestrates sophisticated survival plans. It tries to conserve oxygen by shutting down demanding systems. Essentially, the body willingly creates a 'starvation' mode. In starvation, a process known as ketosis occurs where fat is broken down for energy, producing chemicals known as ketones. This is the fundamental concept of the Atkins diet. Ketosis is also carried out by hibernating animals. It appears likely that ketones have some kind of beneficial effect. And this is true. Ketones are an anticonvulsant, which is why the severity of epileptic fits can be reduced by putting patients on diets. Ketones protect the brain from hypoxia and low levels of glucose. Even sperm are more motile in ketones, and the heart increases its workload. In short, starvation can actually be beneficial. A synthetic ketone is being trialled in adults with heart failure in Belgium, and there are more studies which will test ketone compounds with patients and premature babies. And studies have shown that force-feeding of ICU patients in hospital can lead to muscle wasting, a new method of intermittent, low feeding may prove much more helpful. Perhaps a more modern and effective treatment needs to accept starvation as one of the body's natural defence mechanisms. There's some truth in granny's advice - 'feed a cold, starve a fever'. Ketones, ACE, genes, and fitness. I wondered what would my genotype be. Did I respond to exercise well, like an II, or fall in between, as an ID? I have only ever ventured up a bouldering slope, but I have dreams of climbing Kilimanjaro. How much extra preparation would I need? "Should I take ACE inhibitors to improve my chances of reaching the summit of Everest?" asked an audience member, a self-diagnosed DD. "Yes... but we haven't done the study yet." The study is in the planning stage, but they still don't know how ACE inhibitors will react with the body in hypoxic conditions. This is too big a risk to take on a mountaintop. And throughout his talk, Hugh pointed out that D alleles were not to be perceived as inferior. This is the first gene that was discovered which was directly related to fitness. It has some striking lessons for hospital care. But it is not a case of genetic determinism, stating who is likely to be the best at keeping fit, or surviving overall. The D allele confers its own benefits. People with DD appear to be more resilient to haemorrhage. And they are likely to be stronger, better at swimming and sprinting. They tend to show greater muscle mass in old age which significantly reduces the problems of frailty and falls. I thought of my father, silver-haired and 70-something, still stomping round, still operating heavy machinery, still involved in the mysterious and never-ending movings of heavy objects around his property. For that matter, I also thought of my mother, thin, frail, and disabled, but who has been doggedly picking up an entire bulldozed bungalow, brick by brick, and assembling them into an array of neat stacked cubes in her garden (don't ask). I might never know my genotype for I or D and I might find it hard to predict, but it probably didn't matter anyway for my fitness. What matters is the mind - willpower, determination. For his part, Hugh was vehemently opposed to casual genotyping for these alleles. The research needed to carry on, and it would be too easy for, say, medical insurance companies to jump the gun and draw broad - and expensive - conclusions. After all, for all his incredible-sounding athleticism, Hugh himself is a DD. You can listen to a recording of Hugh's talk here ... And the following questions here ... Hugh Montgomery also talks about his discovery of the first gene for fitness to Jim Al-Khalili, on the BBC's The Life Scientific
0 Comments
 In Amsterdam they are hosting Gunther von Hagens's latest exhibition of plastinated human bodies. Its theme is a universal human quest- happiness. The Happiness Project features six floors of delicately dissected human bodies, bones, tissue, and organs. My first encounter with plastination came when I went to a university open day for Biomedical Science. While one of the professors spoke to us, he held a quarter of a plastinated human head in his hands, absently turning it round and around while he spoke. I could hardly take my eyes off the piece of head. The eyes were closed and the strangeness of the isolated piece of face and brain gave it an almost living aspect. It was not a dead piece of tissue, rather it looked like a perfectly created piece of cyborg, ready to power-up once more if the missing pieces could be plugged back together. There was also a plastinated forearm and hand, skin removed to reveal the wiry network of tendons that usually jerk the fingers back and forth. I was 18 at the time and had never seen human remains, and spent a lot of time afterwards questioning how I felt about those objects. They had been part of people once, they had represented part of an identity. But that had been in the past. As I had seen them that day, and as they would continue to exist, day after day into the future, they were now useful anatomical exhibits. That they were human flesh as well as plastinated polymers and chemicals was irrelevant in that respect. The view was twofold. On one hand, I could invent a backstory for that head and wonder how the man would feel now about part of his visage being preserved for so long, and to be restlessly rotated before a group of visiting school students. On the other, how fascinating that the sticky sclera and soft flesh, so troublesome to preserve and show, could now be safely and cleanly sealed forevermore, odourless and highly detailed, like butcher's meat in plastic wrap, but better. So safe, so free of decay and identity, so scientific. I saw an earlier Body Worlds exhibit in London, in 2009. It had been disconcerting to see figures arranged in classic poses from art and literature. I had thought the plastinated bodies were there to teach visitors about human anatomy, but Gunther von Hagens was also using this new depiction of human form to present themes about the culture and art of humanity. Plaques and captions added snippets of fact and narration on the themes of happiness. The floors represented different regions, from the uppermost cerebral discussions and displays of happiness, with brains and brain slices, to the basement floor of sex.
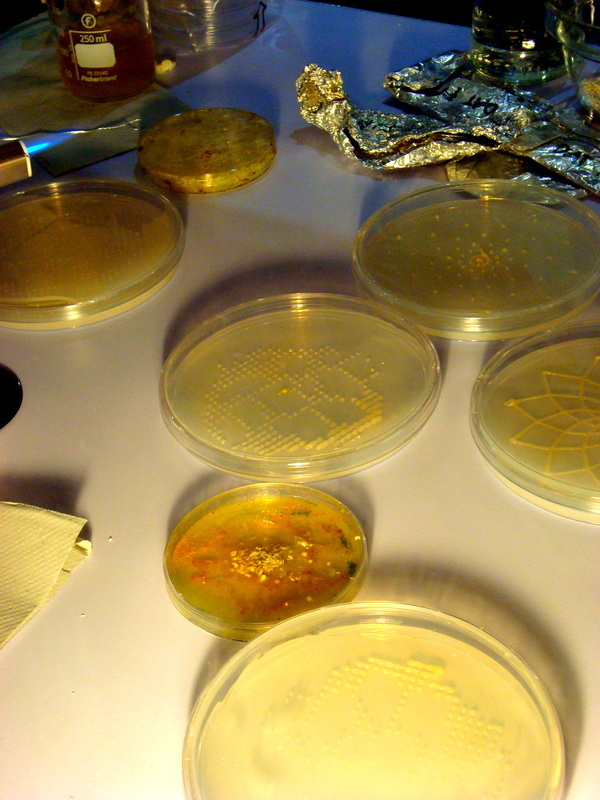
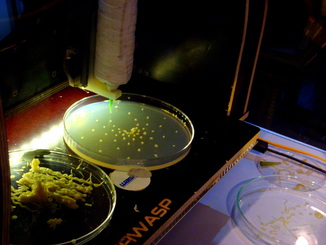
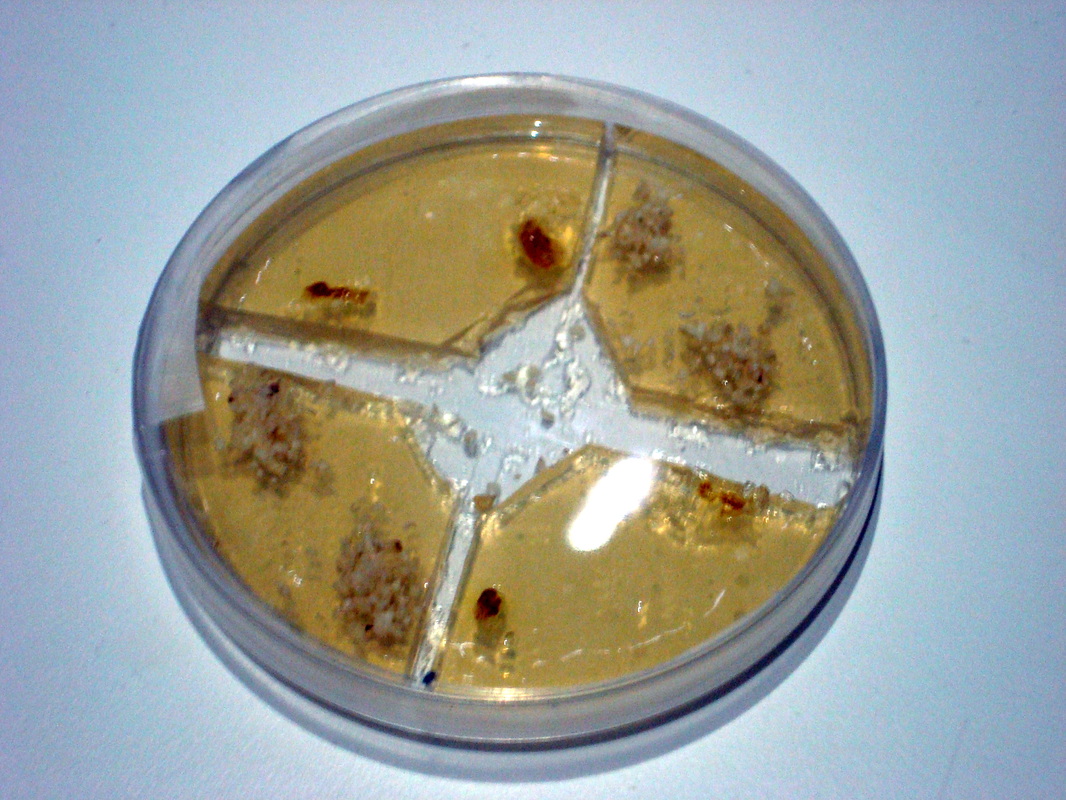
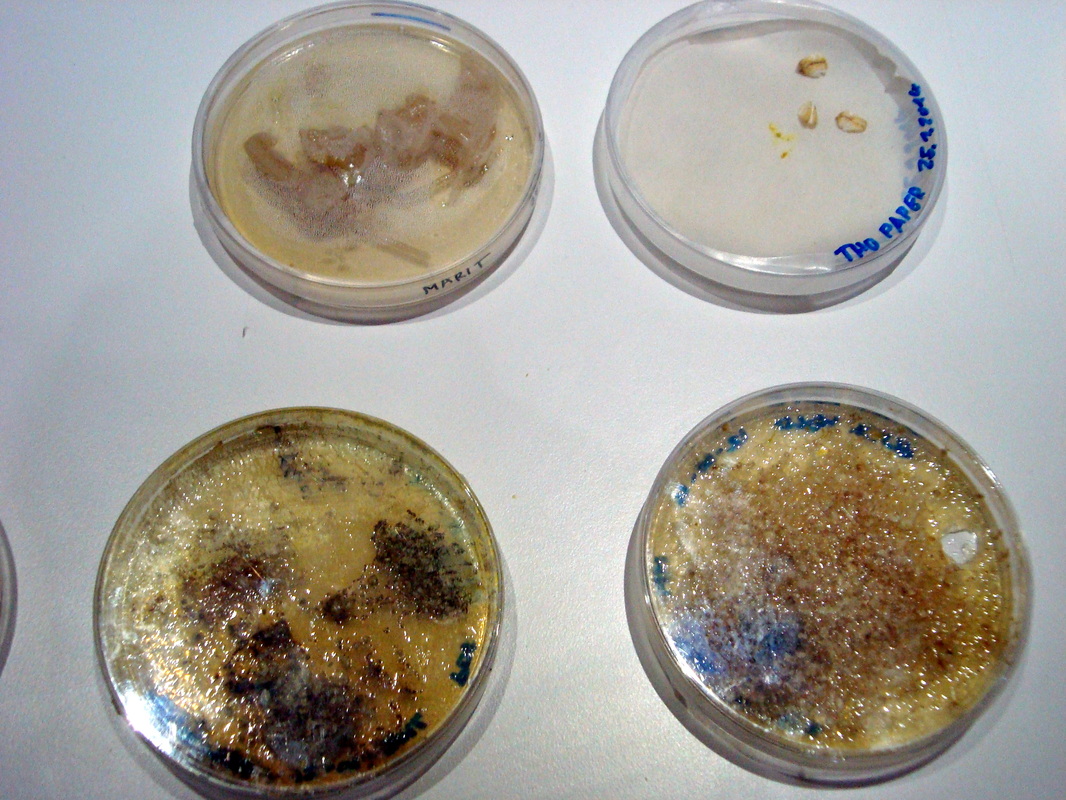
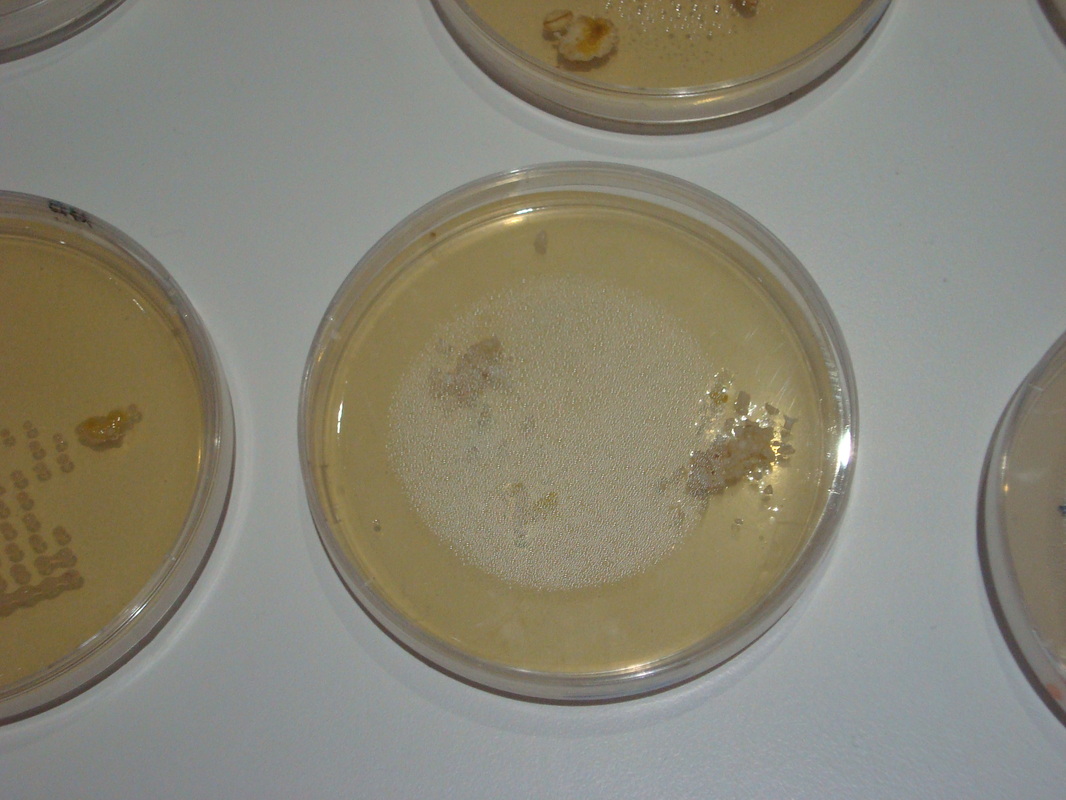
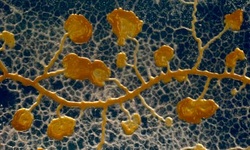 I like slime moulds, and so should you. Let me convince you. Slime moulds seem to bridge the gap between fungi and animals. In a nutshell, they are a glistening goop that spreads and develops in a webbed network of frilly fingers. But this is an intelligent goop. Slime moulds respond malleably to their environment. They can work out the most efficient shape to morph into in order to reach multiple food sources. Scientists have shown this ability compares favourably to some of the most efficiently planned human transport systems. When times are hard, the slimes can change form to produce fruiting spores, sending its spores away to find better lands. When two slime moulds of the same species meet, they join forces into one large super-slime. Best of all, they seem pleasantly benevolent compared to many other microorganisms. No slime mould has yet proved itself to be a human pathogen. And they not only eat bacteria, they farm it. So slime moulds are a wonderful piece of the biodiversity puzzle around us. And we're slowly getting to know more about them. They have cropped up in the 2010 Ig Nobels, for instance. But there are some incredible combinations of man-made technology meeting nature, like fabulously weird experiments using slime moulds as living computing interfaces (quick translation: cyborg technology). Andrew Adamatzky's group at the University of West of England have almost given slime moulds a human face. And on 27th January 2013, I attended an exhibition of slime moulds and 3D printing. It was an interdisciplinary event hosted by the Waag Society, an arts-meets-sciences-meets-design sort of incident. While the supposed schism of the arts and sciences has long been debated and reinvented to zombified death, introducing 'design' as part of interdisciplinary events has crept in on the tides of 21st century technology. The exhibition showcased the results of a two-day workshop where participants designed with slime moulds and 3D printers. This was to be my first visit to the Waag Society, institute for art, science and technology, and I'll admit, I was wary. I hardly knew much about 3D printing on a small-scale, and how could you design with a living organism? To prepare myself for disappointment, my pessimistic mind conjured up images of an exhibition space containing conceptual sculptures splashed 'artistically' with slime mould goop. There might be a lot of dainty talk using inaccessible artspeak. In short it could be all show, no engagement. But there was no need for these pessimistic thoughts. There was plenty of show and plenty of engagement. 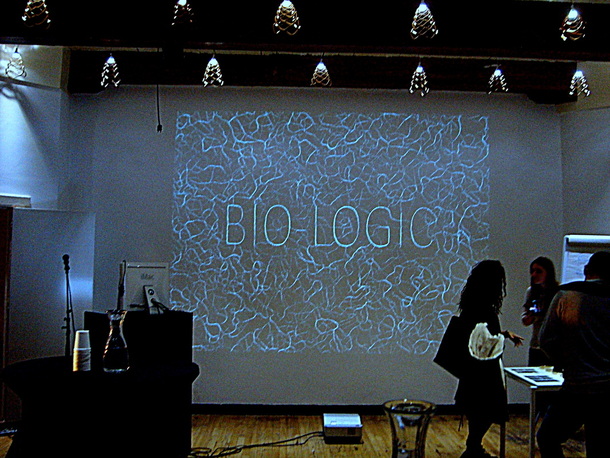 The beautiful old Waag building is an excellent space for science-related public events. The winding staircase, curved walls and old architecture-style is fertile ground for imagining classical scientists pursuing their work. For the Romantics, where else should you be bringing new creations to life, other than at the top of a wood-panelled, historical tower? Indeed Rembrandt immortalised dissections carried out in the Waag. Inside there was a healthy mix of public, scientists, and designers. A few small tables showed the results of the two-day Bio-Logic workshop. A table held a couple of stewpots serving as simple incubators, and another held an array of petridishes containing yellowish agar and seeded with slime mould spores. A few computers with coding programs. A 3D printer in a modified box which served as a sterile cabinet.
Afterwards, scientists, designers and public mingled to discuss ideas and ask questions. I loved thinking of the little flake of slime mould spore material in their dormant state. Ostensibly dry and dead to the eye, but merely waiting. Sensing their surroundings. Unfurling, slowly, responding. Molecular mechanisms begin to cascade, moisture is drawn up. The machinery unfolds. The mould becomes a mobile slime again and reaches for food. I learned more about the slime mould being used, Physarum polycephalum. It can move as quickly as one centimetre an hour. The giant cells it forms are called plasmodia, and contain several nuclei. As in any microbiology lab, contamination is an ever-present problem and can ruin carefully constructed petridishes, but sometimes slime moulds have used the invading growths of fungi as a scaffolding to climb out of the petridish. The moulds can also lay down a trail of physical 'memory'. They can leave crystals behind as chemical signals, marking where they have explored. They can also keep time. When researchers exposed a slime mould to a pattern of regular temperature changes, it learned to anticipate these environmental changes. One visitor asked if the slime moulds could be used to make a 'circuit switch'. And the scientist's answer? Yes! See here for more information. A hacked 3D printer designs structures out of organic material, and the slime moulds redefine these structures. It's a start of a design exploration, bringing together technology and living matter.
So what do these slime moulds look like in action? You can watch a beautiful time-lapse video here. This is about why I went into science communication. It's also about why I studied science. And about why I feel so passionately about visual art. It's all of those things, because I think they come from the same place. On my birthday, I went to Hoge Veluwe National Park in the Netherlands. The park is a beautiful amalgamation of rough green heathland and distant tree copses, red-barked pines and savannah grasslands, African desert dunes and twisted silvered trees. I cycled through and marvelled at how the land changed as I went further in.
And in one wing, the van Goghs. The paintings are laid out chronologically, and feature a lot of early van Gogh. There are examples of the first still-life paintings he produced as he was first learning to use oil paint, in 1881. And several works from 1882-1885, when he was dedicated to depicting peasant life and rural farming. The museum has The Potato Eaters and Loom with Weaver. There are also a few landscapes from this period. Boggy-dark, muted green, obedient in their depiction of reality and technique. What struck me is that, if you associate van Gogh with the most famous and reprinted works that came later, these paintings are remarkably boring. Superficially attractive in their realism, with clues to his style of painting throughout. But nothing that you might not already know about these landscapes, these scenes, these ideas. The Sower, though. I went in close to count how many shades of blue. You can see the same shades hitting the canvas in strokes that might overlap, but which never blend. He didn't smear the colours together, he laid them on. There's a layer of grey-blue strokes, a layer of pale blue strokes, a layer of purplish-lilac-blue strokes. Spattered throughout, shrill dabs of orange. Orange and blue are opposites and so in terms of seeing colour, the contrast can't be greater. And when I stepped back... everything changed. 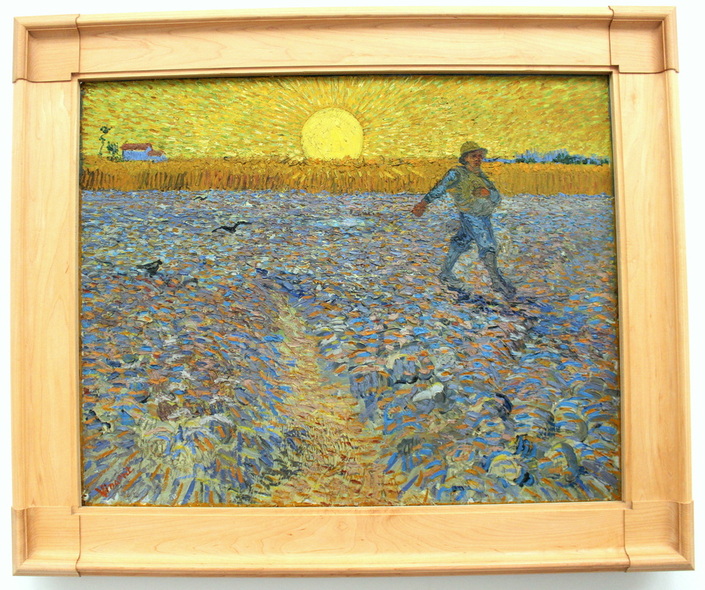 It was then I realised there's an ideal viewing distance for van Gogh's most colourful paintings. It's the point where contrast between blues and orange and yellow start working together. They sink into the eyes. And the effect is like music. Every paintstroke a beat, a note, a particular sound. Taken all together, the contrasts of colour work like a symphony. And in this painting, against everything playing out of the foreground, in the background the linear motion of the sun rays blaze outwards and set a constant tempo. Close up you see the notes, but from further away you can see the full music. And this. Far more beautiful than his titular Sunflowers, that yellowish sunny painting I was first introduced to in primary school. This is Four Sunflowers Gone to Seed. Again, close up I saw the strokes. Stepping away, I saw how everything came together to make four dying flowerheads come ablaze.  Contrast. That's why I like Vincent van Gogh's style, his paintings. I have been thinking a lot about the Sublime, since interviewing Anna Dumitriu about her artwork. If we take the Sublime to mean an incredible beauty, it's something that can only be sharpened and highlighted by contrast. Orange against blue, black against white, paint contrasts etched onto canvas, a symphony of something beautiful that van Gogh saw. The painting was full of movement and direction and tempo. 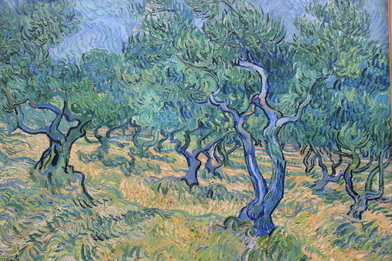 Even van Gogh's life was about contrast. Beauty and darkness, depression and mania. He could see incredible visions of the Sublime in the scenes he painted, of the countryside, of objects, of people, of streets. He painted his excitement and fervour into his works, striking out each piece into a moving orchestra of colours and brushstrokes and direction and tempo and blackness. Then there were the times of horror, of nothingness, melancholia. Perhaps the Sublime comes and goes. Like the sun, you can't stare at it forever. In between the beauty, the ordinariness, and beyond that, the complete lack of beauty.
 I studied van Gogh in high school. The first time I saw an exhibition of his work was as a visiting exhibition at a modern art museum in Seoul, South Korea. What struck me then was the shininess of the colourful paint, which looked almost freshly applied. The chapped texture of the brushstrokes buttering the colours on. They were famous, and old, and alive. And I'd had no idea he had created so many paintings. Like most people, I grew up on a diet of Vincent van Gogh's Sunflowers. The same image turned out and appearing in textbooks, posters, school lesson photocopies, again and again, as though on a carousel.  Colour has always been what I like best in paintings. Colour and contrast. Colour played against blackness to bring it out and make it breathe. Sitting in the museum, staring into a van Gogh painting, I felt an odd feeling, like a brief psychological disjunction. I was reading a message written out in paintstrokes and paintings by another long-passed artist's work. Did I feel as he had felt? Did he know what it was that he created in his work?  Feeling how another person feels, seeing how they see. I thought about this a lot as the museum closed and I started pedalling back through the park. Along with visual art, I have always liked science. I like to know the names of things, and why things happen. I like to see in closer and closer detail how something works, from learning about a leaf, to the cell, to the mitochondrion inside and beyond to where you can no longer see, in the diagrammatic sketching of the visualised electron transport chain. School had always been about progressing in greater and greater levels, so it's not entirely unsurprising that I studied Biology at university. Knowing these things gives me a sense of similar excitement to looking at a beautiful contrast of colours in a painting. And to step back from the details, to try and hold everything in your head at the same time as you look at the bigger picture- how the machinery of the genes moves the molecules that connect up the proteins that altogether animate the entire organism... it's bewildering, and it's incredibly difficult. That's science. But it seemed to me that trying to hold everything together like that is not so different from stepping back from a van Gogh, and finding the point where everything begins to move and work together as one. And that was why I'd become interested in science communication, too. Science communication can have many roles and they are best explored in another article. I'll define two major types of science communication here, though. One reason is to communicate clearly, to rearrange a piece of complex jargon-filled research into something legible to a non-specialist. The second reason is to make you feel as I feel. There's a beauty in science communication, because it is an art form. The way an idea is expressed, whether through words, a picture, a book, a sentence, an article, a concept. If I could create something that communicates that flash of beauty, fascination, of that Sublime in science, then I will have shared what I see in it. And that's the true point of science communication and science engagement to me. If I ever achieve that then it will mean, like van Gogh to his viewers, that I succeeded. “Art is science made clear.”
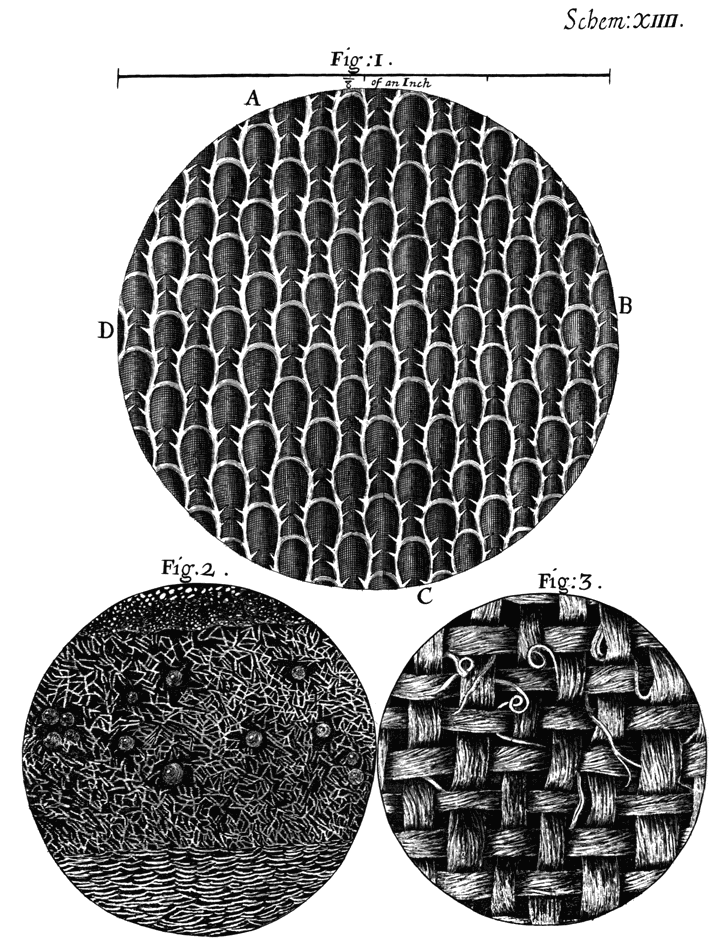
Jean Cocteau - French poet, artist and director Recently I read Imagining Science: Art, Science, and Social Change. The essays discuss a few different themes. There's an essay arguing that art is a valuable tool for anticipating scientific breakthroughs, and opening up dialogue. Some examples include the US President's Council of Advisors prepping themselves for a debate on nanotechnology, by reading Michael Crichton's Prey. Members of Congress also referred to Margaret Atwood's The Handmaid's Tale when discussing reproductive technologies. One might argue their choices of dystopian fiction to open up a reasonable debate on science. While it is a useful thing that imagination can precede scientific discovery, the most exciting stories tend to dwell on the worst possible consequences. Still, that's another point of how art can go where science can't, setting the boundaries for debate by depicting extreme outcomes. A lot of the essays in the book were also obsessed with discussing the differences between 'art' and 'science'. Most of these also seemed to be written by scientists, or sociologists, rarely self-declared artists. And a basic problem was very obvious. When you begin by laying out your definitions of what makes art 'art' and science 'science', the discussion is already lost. It becomes a debate. Art has this quality, which science does not. Science has this quality, which art does not. In struggling to define the qualities of two incredibly complex and varied fields, stereotypes appear and art is painted as mysterious, cultural and dramatic, while science is distilled into methodical, purposeful and clinical. A yawning gulf of difference opens up between the two and the writer has created C.P. Snow's two cultures anew. One writer described his experience in a particle physics laboratory. "Nobody in the lab made any reference to "beauty" in the construction of an experiment. Nobody mentioned how "feelings" shaped their work." He compared this unfavourably to his wife the painter, and the emotional reactions of people viewing her paintings, and declared an inherent and fundamental opposition in art and science. "Given all this, what I find quite amazing is the notion that artists and scientists would have much to say to one another in any realm." Another writer also emphasised a mutual exclusion of science and art. "Science is a system" whereas "Art has no agreed upon definition... It admits the possibility of nearly anything." Collaborations of art and science are "more expressive of a desire than logical possibility" and art cannot engage science, it can only engage the ethics of science. (Art, Science and Aesthetic Ethics). After a few essays like this, a person could be forgiven for thinking of science as a land of ice-hearted joyless automatons obsessively reducing the world into finer and finer slices of truth with high-powered technology, while art is a land of empathic flighty navel-gazers whose rocking hammocks are gently powered by the joie de vivre bursting from their indefinable hearts. So what do I think? I think it is all relative. To begin with, to be able to write about art and science, you must have some concept of what kind of art and what kind of science you are addressing. Do you have products of art in mind, exhibitions, theatre, paintings? Or are you thinking of the theory of art? Art defined as inspiration? Science meaning factual knowledge? The scientific method? There's never going to be much definitive progress on discussing art and science without first defining what it is you mean by art and science. Even essays that ostensibly hold similar viewpoints in the book may not, because they start off with different pieces of the concepts in mind. Now for myself, I generally take art to mean a sensation, a feeling. I am unashamedly going off my own personal experience here. To create something with your own hands. To look at a blank canvas and start transferring an internal mental vision onto the expanse of nothing. To hear a piece of music and be struck by a rush of feelings, of inspiration, a sense that something has been invented in your head which was not there before. I suppose some might call my definition of art creativity, but I think creativity describes rather the process, while art is the way of seeing, feeling, and thinking. To strip it down further, I could suggest it's about seeing beauty. And of course beauty is subjective, but I've already written about seeing the Sublime in Van Gogh's paintings, and how I found the sensation to be the same as when I learned science. I can't be the only one. Those particle physicists in the laboratory are not automatons, they would have gone into science because they saw something beautiful in it. Everybody is a scientist and an artist. Perhaps it is only less obvious because the skills used to capture art are more obvious in some forms than others. Van Leeuwenhoek made his microscopes and selected objects to study with them quite randomly. He was motivated by a love of what he saw. He used his drawing ability to express his love of what he saw. The father of the neuron, Ramon y Cabal, also saw the art in the brain cells he examined. He also happened to be interested in photography and painting. His photographs and drawings express his interest...(etc). The Origin of Species is elegantly written using that artistic medium, writing. Part of the reason that the Selfish Gene has generated such furore is because the scientific concepts within have been so clearly expressed. I don't like to set up these two concepts like two sides of a chessboard. On one side, we have Science. The other, we have Art. Media loves this false dichotomy for the easy reactions it invokes. But there's such a basic problem from the start in setting up two different items as discussion points. The instinct is to define each one by their uniqueness, and their difference from the other. Set them at odds. Make sure no progress is ever made. What is the romantic disease? Watch the film below to see artist Anna Dumitriu talking about her exhibition. 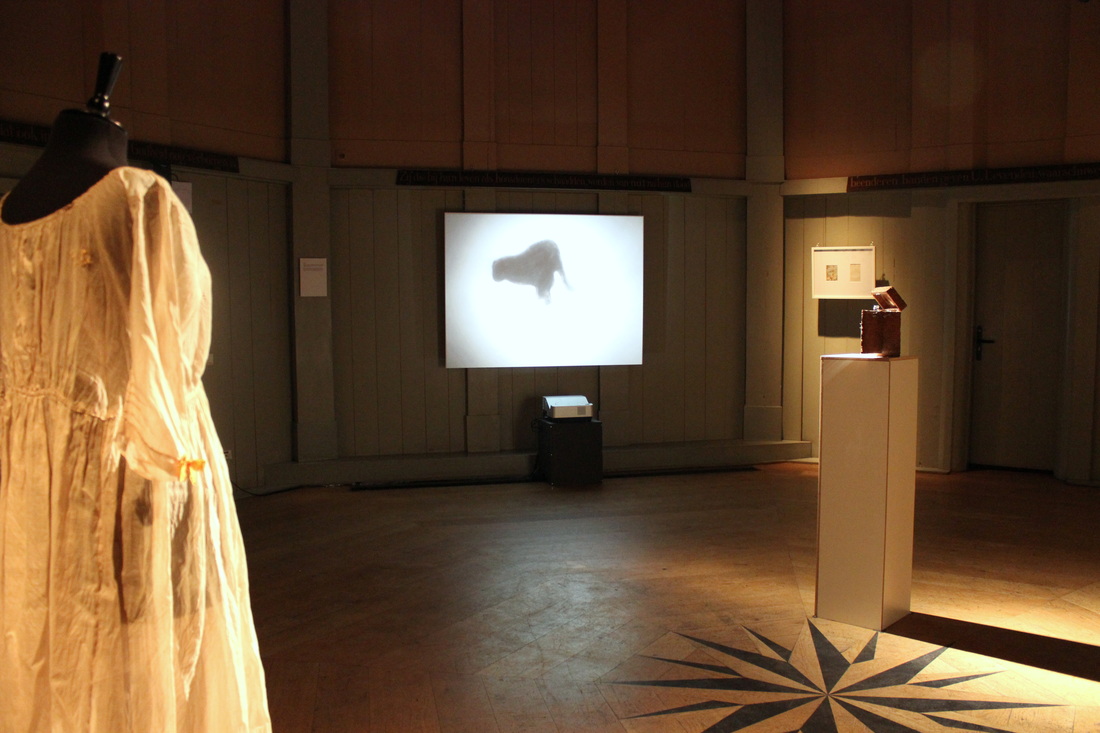 Anna Dumitriu explains the stories behind her exhibition here I’m in a room with humanity's biggest killer. It began eating away at us over 9000 years ago, and has never really stopped. The marks of our relationship surround me in an array of medical leaflets and dyed fabrics. Mysterious objects sit on stands. A glistening set of metal needles and devices inside a spongy wooden case. There's a tiny, bare bed, and a ghostly pale dress. A collection of tiny felted grey lungs that resemble a group of settled moths on a wall. This is an exhibition on tuberculosis. 'The Romantic Disease' has been created by Anna Dumitriu, a British artist with a taste for microbiology and emerging technologies. She is the artist-in-residence for the Modernising Medical Microbiology project, a collaboration between Oxford University and Public Health England, and she was inspired to create this exhibition by their research into bacterial diseases. The exhibition is on tour through Europe, and is currently hosted in the Theatrum Anatomicum at Waag Society in Amsterdam.  What caused tuberculosis? On one side of the room I see an animated black dog circling and pacing endlessly. It represents one early interpretation, the 'demon dog'. This dog would enter the bodies of sufferers and bark, making them cough. Later, people thought tuberculosis could be inherited. On another wall I read an old medical text warning of the 'tubercular taint' that could be passed on through risky marriage. I find out that the pale dress hanging on its stand is a Romantic era maternity dress, representing how some pregnant women with tuberculosis were forced to have abortions. It was a long time before the real cause was found. Bacteria were only seen for the first time in 1676 by Anton van Leeuwenhoek, and in 1882 the microbiologist Robert Koch proved that tuberculosis was caused by bacteria. 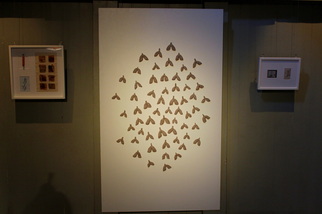 At the entrance to the exhibition I spy a quote from the Romantic poet, Lord Byron. ' “How pale I look! – I should like, I think, to die of a consumption –because then the women would all say, 'see that poor Byron- how interesting he looks in dying!” ' Ah, the vanity of poets. I wonder how tuberculosis could ever be thought of as 'romantic'. The disease was called 'consumption' from the 14th century because of its vampire-like effect on sufferers. It mainly eats away at the lungs, causing hacking coughs and bloody sputum, sweaty fever, the body weakening and wasting away. The statistics for tuberculosis are shocking. One third of the world's population are infected with Mycobacterium tuberculosis, the bacterium responsible for causing the disease. Of those, ten percent will develop the disease. Of those, around five percent would die of it without treatment. It is currently the second most deadly infectious disease after HIV and has killed far more people overall. While it is curable with modern antibiotics, in the right conditions extremely drug-resistant tuberculosis can evolve. So what's romantic about all of this? But I'm looking at this wrong. Nowadays, we know about tuberculosis. We know about bacteria. We have antibiotics and medical advice. We have scientists with gene sequencers and electron microscopes. But for most of our history, people did not know what caused, spread, or cured tuberculosis. Forced to live alongside this mysterious and widespread disease, unpicking its mystery with slow science, people also responded with myth, imagination, and art. After all, anyone could get tuberculosis, from famous figures to the unknown. Many Romantic Era artists like Keats had it. Perhaps Byron spoke tongue-in-cheek, since his own father died of the disease. And unlike other common diseases of the time, like smallpox, tuberculosis was less devastating on the appearance. A waifish, pale appearance was even considered fashionable, tuberculosis or not. This is not so different from today's unchanging fashions of the catwalk, or tastes for sparkly skinny vampires, then.  And while many artists had tuberculosis, could tuberculosis actually create the artist? Some people have theorised that tuberculosis enhanced creativity by inducing spes phthisica, a state of euphoric creativity before death. While it's likely that this state was only based on romantic anecdotes, perhaps a feverish delirium could inspire strange and artistic ideas. Anna showed me around the exhibition, inside the softly lit circular room of the Theatrum Anatomicum. Her artworks tell the story of how we have long tried to understand tuberculosis. “Because it's had such an impact on humanity, there are a lot of myths around tuberculosis,” Anna says. “And there's a lot of different areas of medical research that have changed over time. There's this fascinating cultural story alongside the microbiological side.”  How was it transmitted? “Where there's dust there's danger,” warns a 1902 guide by the National Society for the Prevention of Consumption. At this time, tuberculosis was thought to be spread mainly by infected spit that dried on specks of dust. Invite a few tuberculosis sufferers into your home, let them spit on the floor, neglect to sweep for a few weeks, and eventually you could be stirring up clouds of death with your broom. Close up, I see the moth-like objects on the wall are actually tiny grey lungs. These are made from felt and dust, by Anna and people who have attended her interactive workshops. The advice was almost right in that tuberculosis can be spread by sputum, sprayed into the air by coughing, but dust could not spread tuberculosis. Drying out sputum droplets tends to kill the bacterium.  Today, thanks to whole genome sequencing, transmission of a disease can be more precisely mapped. I learn about this by examining a stand holding an old 'pocket-bottle for coughers'. The Blue Henry is an attractive blue glass bottle with a silver lid, intended to provide a safe and fashionable receptacle for sufferers to cough up blood in public. Like many of the artworks on display here, Anna has combined the past and present of tuberculosis on this object. The top is engraved with a patient transmission map, produced by the research of the Modernising Medical Microbiology (MMM) project. Today, the MMM scientists investigate deadly bacterial diseases by sequencing the genomes of the bacteria responsible. Using the sequences, they can identify which strains are responsible for disease outbreaks, and they can also map the transmission of an outbreak back to its source. The diagram on the lid of the Blue Henry shows how multiple people were infected by one person, who was in turn infected by Patient Zero, the first person to get the disease. Prior to whole-genome sequencing, unravelling the spread of a disease would have relied on a laborious process of interviews and piecing together likely infection scenarios. How was tuberculosis treated? There are fascinating items showing how tuberculosis treatments were marketed. 'REST... to beat TB' one medical poster declares, showing an improbably merry man as he lies in bed, resting off his tuberculosis. Resting was supposed to help recovery by lowering the breathing rate and giving the lungs of sufferers less work to do. Patients would also be shuttled off to sanatoriums in mountainous regions, where the air was thinner and thought to be better for the body. Anna tells me about an infamous Welsh mountain sanatorium, Craig-y-nos, where children were forced to sleep outside in fresh yet painfully frosty air, since this was thought to be another benefit. A jaunty magazine poses an attractive young couple under the headline, 'I had TB!'. Below this, Anna has arranged an innocuous little microscope slide of stained M. tuberculosis from sputum, the foe in question.  But there are also works based on more sinister tools. Anna explains that artificial pneumothorax- collapsing a lung- was once a common treatment. The idea was that collapsing the lung would 'rest' it, giving the lung a break to tackle its tuberculosis infection, and also starving the tuberculosis bacteria of oxygen. Around one third of tuberculosis patients were treated to this between the 1930s to 1950s, including the writer George Orwell. It's a toe-curlingly unpleasant idea, but Anna tells me that some small, recent trials suggest this antiquated treatment might help fight the modern rise of extremely-drug resistant tuberculosis. Sometimes medicine, like history, turns in cycles.  Textiles and dyes also play a large part in the history of tuberculosis. The maternity dress has been dyed with walnut husks, madder root and safflower. All common natural dyes, and all early treatments for tuberculosis. There's a vial and fabric-stains of Prontosil, the world's first 'sulfonamide' drug which could slow the growth of bacteria. It was produced by Bayer, today known as a chemical pharmaceutical giant, but who began as a dye manufacturer. Bayer's large chemical laboratories for producing dyes were perfect playgrounds to test out new chemical combinations. With ready supplies of coal tar, a by-product of coal production, a base for many dyes, and the bane of my childhood thanks to my dad's inexplicable fondness for coal-tar soap, many scientists tried to produce dyes to specifically target bacteria. Along with other useful products like aspirin, Bayer eventually produced Prontosil, and medicines derived from this bright red substance were widely used in bandages during WWII. It also had the side effect of dyeing the skin red. Anna has also found staining effects in modern treatments for tuberculosis, and she used the growth media for Bacillus Calmette-Guerin (BCG) (an attenuated strain of Mycobacterium bovis used as a vaccine for TB) to add striking touches of pale blue to some of her artworks.  I also find out that Byron's vain wish to be pale and interesting would get a colourful update. Anna reveals that a modern antibiotic used to treat tuberculosis, rifampicin, can cause the tears and sweat to turn orange. “In a way, they look like they have a nice tan,” she commented wryly. “So it's interesting how that link between fashion, appearances and tuberculosis has come about again.” Stories and the Sublime Anna is fascinated by objects that are tainted with the story of the disease, and has added more subtle combinations of old and new stories. The dress and tiny lungs are infused with the extracted DNA of M. tuberculosis. There is no danger that the DNA can harm anybody. But the DNA's presence in objects so close to me make me feel face-to-face with the bacterium itself, laid open before me. It is an intimate and respectful meeting, one without infection, disease, or pain. “My research into this exhibition began with conversations with scientists, and reading about the disease, and the more I did the more stories I found. The strangeness of everything, the stories, it's not really what people expect,” reflected Anna. “I'm definitely planning to take the work further, I think there's many more stories to be told.” She also runs hands-on workshops to explore the history of tuberculosis further, and sometimes people attend who have experienced old tuberculosis treatments first-hand.  Looking round the exhibition, I'm struck by how much it has filled in the cultural side of tuberculosis to me, something which was entirely missing when I studied the disease at university. In modern times we might easily think that only the scientific view remains now. With sophisticated technologies or new drugs, scientists work towards understanding cause, transmission, and treatment in ever closer detail. But cultural understanding of the disease is something uniquely human. And inspiration and appreciation of the microbiological world play a vital role in pushing scientific discoveries. Anna points out that microbiology is still a relatively new science. It was only a few hundred years ago that Anton van Leeuwenhoek, a textiles dealer, first saw microbes under his homemade microscopes. Van Leeuwenhoek was not a scientist, he was a textiles dealer used to examining thread counts under magnifying glasses. Yet he was inspired to explore the microscopic world after seeing pictures from Robert Hooke's 1665 book, Micrographia, with its detailed illustrations of textiles in the microscopic world. Van Leeuwenhoek went on to make a number of groundbreaking discoveries in science, and was always guided by his interest and appreciation in what he saw. “We're at a fascinating time when new technology is available and revealing more about the microbial world,” Anna said. She is also looking forward to exploring our relationship with other infamous bacteria, including artworks based on Staphylococcus aureus, the agent responsible for MRSA.  I asked Anna what she wanted people to go away from the exhibition with a sense of. “To me bacteria have this effect of the sublime. With all the effect they've had on humanity, but the fact that they're fascinating and beautiful too. Ideally I'd like people to come away from the exhibition with a sense of the bacterial sublime, to understand the sea of bacteria they're a part of, and that they're super-organisms containing bacteria. I'd like people to understand that.” 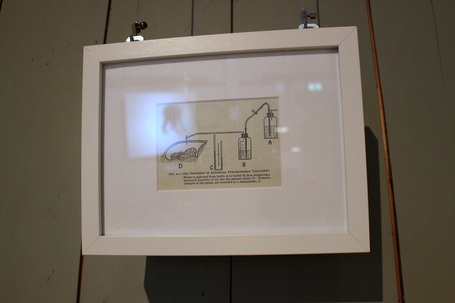 Additional Information
Anna Dumitriu explains more about her artwork and inspiration in this film. Anna Dumitriu received a Leverhulme Trust Artist in Residence Award in 2011 to work with the Modernising Medical Microbiology project led by the University of Oxford, Nuffield Centre for Clinical Medicine, in conjunction with Public Health England. 'The Romantic Disease' exhibition is funded by the Wellcome Trust. The exhibition will be shown at the Waag Society until 27th July, and the Art Laboratory in Berlin from 26th September - November 2014. Links Anna Dumitriu's website: http://normalflora.co.uk/ Modernising Medical Microbiology website: http://modmedmicro.nsms.ox.ac.uk/ Waag Society: http://waag.org/en/event/romantic-disease-exhibition Further reading
I'm watching a man play music with his butt. When I woke up this morning, I had no idea my day would end like this. 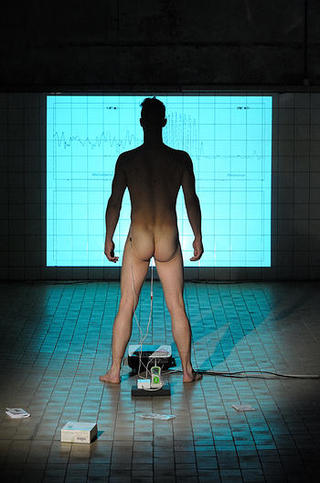 (c) OCNM Archive / Martin Popelár We the hushed crowd examine the large projection before us. Dani Ploegar stands naked and proud on a blue-tiled floor, his back turned towards us, the top half of his body cast mysteriously in silhouette whilst a soft, gold-tinted light frosts his legs and muscular buttocks. In his butt he has secreted an Anuform anal electrode, and falling away from that hidden egg is a long cable connected to a modified Peritone EMG sensor. These commercial medical devices were developed to treat incontinence by enabling users to exercise their rectal muscles. But Dani is using them for art. He is working his sphincter to a specific beat, performing an extremely rare combination of falsehood and carnal pleasure. For he is faking a male orgasm, clenching his muscles to mimic the rhythmic contractions of pleasure, which Anuform and Peritone channel into a synthesiser to produce digital sound. Whooping wails and musical howls warble out from the sound generator, the sound of alien tentacles mopping a floor of microphones, an electronic heavenly chorus in grief. His performance, Electrode (2011), is unlike anything I've ever seen, heard, or considered before. But how does he know how to move his butt? Dani is actually replicating a recorded sphincter contraction pattern from an anonymous male subject, who duly masturbated himself to orgasm as part of a 1980s study. Dani, a performance artist and lecturer at the Central School of Speech and Drama, subverts the scientific data and devices into something new and unforgettable.  It's so bizarre that we are all quietly awestruck. And I love Dani's earnest and serious delivery as the man himself talks to us here at the Waag Society in Amsterdam, a public institute to explore science, art and technology. It's another pleasant and crowded Do-It-Together Workshop, and tonight's topic is Neuro Cyborg. Now that the bizarre has truly been crossed, there is nothing else to do but lean back and appreciate the art. I've already done my bit earlier this evening. I made an insect biomechatronic.  The evening had begun with a quick introduction to brain imaging by Martijn Steenwijk, PhD student at VU University Medical Center. Martijn, a specialist in medical imaging of the brain, explained some of the technology used today to look into the brain's activities. It seems to me, naive 80's child, that imaging technologies have been used for years to peer into the brain. The images are still fuzzy and no one can be quite definite what an area of brightly lit activity really signifies. But bit by bit, there is more to be said from the pictures, because there are more ways to string the data together. While working for the European Grid Infrastructure I have learned about the development of The Human Brain project, a virtual brain that will be built using colossal computing power and data from thousands of brain scans. It is clear that supercomputing is the crucial tool to tell us more about the brain by building a working simulation of nerve impulses, not just new scanning technologies to read the brain's shape and activities.
 Next we had the opportunity to explore neuroscience ourselves, using the Do-It-Yourself kits of Backyard Brains. Backyard Brains are a start-up group of scientists and engineers, who have created a variety of mini-science kits for students and DIY Biology enthusiasts. The kits can be ordered online and aim to deliver 'Neuroscience for Everyone'. You can, for instance, order a 'Spikerbox' to listen to nerve impulses or make a cockroach leg twitch in time to an iPod track. You can also create a 'RoboRoach', a $10,000 project that was funded through Kickstarter, which lets you control a cockroach with mobile phone. To make a RoboRoach, you essentially have to cut some bits off a living cockroach and connect its body to some small circuitry and wiring which will convey electric impulses to the roach's nerves. The fact that the cockroaches don't feel pain provides a sop to any uneasy feelings an experimenter might have about doing this, but the concept remains somewhat unpleasant- and so it should. Nobody should experiment with animal models lightly. The launch of the RoboRoach kit generated controversy, and the creators responded to it. “I try not to downplay the fact that in science we use animal models and a lot of times they are killed,” said Greg Gage, one of the co-founders of Backyard Brains. He also points out that the kits teach about the care procedures of scientific animal models. How to anaesthetise the animal, and how to minimise damage from wounds. And when to retire a model to live out its life, or perhaps, be euthanised. Still, Gage acknowledges, “we get a lot of e-mails telling us we’re teaching kids to be psychopaths.” And a quick google shows me plenty of critical news reports lambasting the RoboRoach. Though I see similar arguments employed in each one - the 'wrong people using the wrong treatment', the slippery slopes of 'roach today, human tomorrow', the general unease of making live animal experimentation into a commodity, even if it is a learning tool. The condensed version is this: if you make these kits available to anyone then someone is going to abuse the science. It's the same popular argument deployed against citizen science, biohacking, and DIY Biology movements. While I don't want to dismiss it out of hand, I do think it obvious that with a few replaced words, that dire warning becomes applicable to any field. If you would like to decide for yourself, you can start by watching Greg Gage's TED talk on the RoboRoach, replete with a live demo.  As the talk finished and the practical part of the night began, I found myself at a table with a Spikerbox and a small tank of roaches. We were to cut off a roach leg and use it to listen to nerve impulse 'spikes' using with a neuron amplifier. Someone fished out a roach and dropped it in ice water to knock it out. I shared nervous grins with the others. Who was going to be wielding the scalpel?  I found myself volunteering. First, I found I wasn't squeamish - I was interested in the science. Second, having handled scalpels and done dissections before, I wanted the responsibility of looking after the roach. Stunned by the ice water, it wasn't going to feel a thing, and provided I cut it in the right place, its only injury would be one missing leg which would grow back within a few weeks. I donned my gloves, picked up a scalpel and zoomed in on the unconscious roach. A few motions, then the roach was put back into the tank to wake up. I hoped that tank life was easy enough to outweigh any living difficulties it might encounter, with one less leg. We then secured the two Spikerbox electrodes into the neuron running through the leg, and plugged the Spikerbox into a smartphone with the Spikerbox app. Manipulating the hairs on the leg tip sent an electric nerve impulse rushing up the limb and past the other embedded electrode, resulting in a crackling and visible spiking depicted on the smartphone. And it really was amazing, to hear a nerve impulse and see it dance upon the screen. We living, conscious beings were all standing around marvelling at simple roach leg nerve impulse thanks to millions of impossibly complex nerve impulses firing in us so we could do the marvelling... but it was the simple roach leg set-up that truly summed up the power of nerve impulses. We jostled for the toothpick to touch the leg, and hear the sound of neurochemistry.  Over on the RoboRoach table, they weren't faring so well at attaching the necessary parts to the roach. Unfortunately, that was one experiment that we didn't get to see. Elsewhere, another table used a Spikerbox to measure human nerve impulses, and then Dani delivered his talk on his sphincter music. After Dani, the final artist was Arthur Elsenaar, presenting Artificial Facial Expression, or Artifacial- a bizarre series of computer-controlled human expressions. Instead of sending bodily nerve signals to an electronic device, like Dani, Arthur inverted this pathway by letting a computer program control his facial muscles. Little electrical impulses are delivered to electrodes patched onto his face and generate a slew of grimaces and twitches. I stared and wondered what on earth this particular juxtaposition of control, electronics and living flesh heralds for our future. I had never considered that we might voluntarily allow robots and electronics to control us, rather than we control them. Then again, isn't deep brain stimulation via electrodes already a pioneering treatment for Parkinson's disease? But what about robotic science and artistic performance? Actually, as Arthur could tell you himself, electronic body performance dates back to the 18th century.  Later on, I cycled back home through the dark streets of Amsterdam. I was thinking, variously, of a cockroach leg, a musical butt, and a computer's face.
 Ah yes, dentists.
I think it's one of those flipside benefits-and-problems of being an adult, that you probably don't go to the dentist as much as you did when you were a child. If you're British, you may not go for check-ups so regularly because it's no longer free on the NHS. Of course, perhaps you also don't eat as many sweets anymore, and no longer need all those shiny silver fillings. Perhaps you don't need Mr. Metal Pick yet for wincing cavities, blazing abscesses, and mysteriously missing teeth. And if you're lucky, perhaps you never will. Good old fluoride in the water. However. If you don't go to the dentist regularly, the following two points apply. 1) You avoid the dentist, and all their little discomforts. See point 2. 2) The dentist is now very, very scary. These thoughts occurred to me as I frowned over the question, 'When was your last visit to a dentist?' in the reception of Amsterdam Dental. I retracted my memory by a few years, counting through Christmases. It would have been around that time, since that was when I would be spending the most time at my parents' house, and my dad, for all reasons previously stated, would have suggested taking a trip to the family dentist on his reasonable NHS rates. Not much of a Christmas treat, I once thought, but I have changed my mind since. Let's continue. -December 2011- I decided. It was probably right. An error margin of a year or so. It was always going to be far too long ago. Guiltily, I also admitted that I did not floss - I had decided to start doing it last autumn, but I had promptly lost the conveniently tiny box of floss I bought, and never bothered to buy another one. In the household I grew up in, flossing was outlawed by our unique family snobbery. Like buying any other toothpaste than SR Mentadent, shampoo that wasn't Vosene, or soap that wasn't Imperial Leather or - god help me - Coal Tar, it was designated as something for foolish people. Finally, I rated my smile as a '4' on the 1-10 scale. Crooked teeth, you see. I handed the form back in, and the experience began. Since my trip here, people have asked why I went to this specific dentist, an expat himself, instead of a Dutch dentist. Honestly? His website seemed good. And he offered consultations on both dentistry and orthodontistry, both of which I wanted consults in. Having to get health insurance in the Netherlands had nudged me into pursuing a general health overhaul. I decided I would get my missing filling replaced, get braces for the second time in my life, an eye test and prescription update, maybe even a health check. This chap had degrees from Harvard and a membership of the American Academy of Cosmetic Dentistry. And a few expat forums recommended him. So there we go, and there I was. The dentists' office turned out to be pretty small and dingily lit. There were three people working there, Dr. T himself, another female dentist, and the receptionist. All three were having lunch behind the reception desk when I walked in. Setting the scene for the entire experience, all three kept eating as I stood there, wondering why it wasn't bright and white inside, like I thought all dentist offices were. Through mouthfuls, the receptionist bid me to fill in the form. Form filled, I went to the adjoining backroom and obligingly hoisted myself onto the creepy dentist chair, a hundred memories of increasingly uncomfortable consults beginning to trickle rapidly through my mind. "So you have a filling that needs replacing?" said Dr. T. He didn't seem sure of what I was there for. But overall he was a casual, friendly figure. As it turned out, way too casual. Nonetheless, I wondered uneasily if I was their only patient at the time for a reason. "Yes. And I'd also like to know about getting braces, as my teeth are crooked. I think I'd have to have some teeth taken out..." "I try to avoid removing teeth. That probably won't be necessary." Really? Actually, I'm not that attached to my teeth. I could easily stand some detachment. There are too many of them, even after a set of extractions. And they're big. My Asian mother's genes daringly bucked the ethnic trend by delivering fairly large teeth. And my dad's teeth... well, he's British. They were never going to be easy teeth. "Bite?" Dr. Tsang offers. I close my teeth in a grimacing grin and show him. He looks at them from a couple of metres away. "No, it won't be necessary." "Oh, okay." I feel disappointed. After a few seconds, I ask. "Are you sure?" This becomes something of a theme throughout the session as I find myself essentially goading him to remove some of the damn things. I am not an expert in giving dentistry, only at receiving it. As the owner of these teeth, I know that there is very, very, little space in this mouth for teeth to get pushed around. Dr. T remains completely laid-back about the whole affair, and completely unwilling to discuss removing any teeth. He actually seems completely uninterested in the whole topic of braces. He approaches to take a look at my missing filling. Now, the fear. Why is it that the dentist was so less frightening when I was a kid? I suffered all kinds of indignities back then without batting an eyelid. I had numerous powdered dry blue rubber fingers poking into my mouth, drying out my lips and making those irritating little rips in the stretched lips that take ages to heal. So many fillings that the numerous different pitches of drill sound darting in and out of my mouth became a drill-bit symphony of high toned wheees and gritting brrrs. Weird tasting powders, fiery liquids, strange ray guns, x-rays requiring bizarre mouth-pieces and awkward hunched positions over sternly cream-coloured machines, blue rubber bibs, the rapid-fire chatter of numbers and oddly scripted-sounding inane chat firing over my head between dentist and dental nurse. At least once during casual check-ups, the dentist suddenly rammed a wobbly milk tooth right off its bed of dangling but tenacious flesh roots without warning. I had a battery of injections into my mouth, including two painful ones deep into the soft tissue of the back of my gums where numbing gel does not help at all, before having four teeth bodily jerked out with what felt and looked very much like a metal car wrench, jets of blood hoovered cheerfully up by slurping pipes operated by the closely peering face of the nurse, raw gums and red nerves exposed to my childishly interested tongue. I had tight metal covers rammed around my rear molars, wire faces welded to my teeth, heat-sensitive wire ratcheted up to unbearable tightness along each layer. I had - and this was my big, shameful secret - headgear. I wore it at night for over a year and every morning the first thing I would do would be to yank the painfully hot spikes out of my aching teeth and fling the whole contraption as hard as I could into the farthest corner of my open wardrobe. Believe me, I do mean every morning. I had all that... ...and I was never scared. Heck, the only time I cried was after one session with the orthodontist, after he'd finished equipping me out with a full set of metal, put the headgear on me and casually demonstrated to my dad how it would pull back like this! like this! on my indignantly screaming teeth... ...and now, lying flat on the chair, mouth held open, I feel like I'm engaging in complicit torture. I am offering myself up as the victim. I have my hands folded across my stomach and my rigid nails digging as hard as they can into the backs of my hands. If I break the skin, the pain will be a welcome distraction. Sweating in fear, I watch as the dentist bears forward. Any second now he will use the tool I have come to fear and hate the most- the metal wire pick. First, though, Dr. T casually operates his little mirror in my mouth. He does this one-handedly, and without the close-lean-in-an-inspect that I'm used to. Is this a sign of professional ease, or just carelessness? One side, the other side, and he delivers a few short comments. "Oh yeah, I see the hole. It's pretty deep." He takes the metal pick and pokes it in. The feel of that skittering little wire haunts me in my nightmares. It makes my toes curl in horror and my skin dampen with sweaty fear. Mercifully, my tooth seems entirely insensitive and dead to pain. Mind you, maybe it is dead. I've mentioned my wisdom teeth as another potential problem. My British dentist had suggested it was possible I'd have to have them removed. Again, my thoughts on this topic has always been very amenable to that idea. I don't need wisdom teeth, I have more than enough in here already. Like the rest of my teeth, the damn things crested early, too. Take them out! "Oh yeah, one wisdom tooth is impacted. You might have some problems there as food can get stuck... cause a cavity." That's all he says. He does some x-rays. It is novel that I don't have to get up. He has a moveable x-ray machine that he pulls down and prods into my cheek. Then he calls the other dentist to come in and do the filling. "You know you can send me any questions you like about braces," he adds, turning to leave. I have to quickly call him back to get my 'consultation' in orthodontics. I winkle information out of him. Like eating winkles, it is an unnecessarily complicated procedure for very little reward. Invisi-align braces won't work, because my teeth are too crooked. I wonder if this is why Dr. T seems so bored when talking to me about braces. Perhaps he is 'Invisi-align' only. Anything else, no thank you. Wire braces will be the best bet, this is fine with me. I ask him about prices. He manages to evade the question. "Won't my teeth just move straight back into crookedness after braces, like when my wisdom teeth crested? I mean, I don't even understand why they went crooked after I had all that work done..." "There's, like, fibres, that hold your teeth in place," he says. It sounds like the sort of easy explanation he could just be making up to placate an idiot. "That's why they can go crooked. So you'll need to wear removable braces for a long time." "For all my life?" Again, somehow, he doesn't answer the question. "It's like, you know, I tell people it's like wrinkles. The fibres. They just happen." The other dentist enters and takes over. Disinterested Dr. T is ready to leave and let the other dentist do the filling. They do, however, first spend a few minutes clattering around with equipment. It's pretty obvious this is not a smoothly running affair. Bits of things are missing. There are questions from her to him about what to use. Drawers are opened and shut. The other dentist searches for things. I think longingly of the cold clinically sterile room of my British dentist. The neatness of it all. The shiny white surfaces. The lack of scrabbling for the right equipment. Suddenly, I miss him. Suddenly I love him. There is a cobweb attached to the light bulb in the ceiling. A slurping tube is hooked over the other side of my mouth, which turns out not to work particularly well, so I have to swallow at intervals or risk choking on water and tooth enamel dust. When she can put the drill down, the dentist helps by sticking another suction tube in to save me from swallowing or coughing. But she only has two hands, and it's either drill or suction. It's a far cry from my dentist and his ever-present assistant. For the first time, I wish there were two sets of hands tending to my mouth. What on earth did I ever complain about? She has a really, really good go at my cavity with the pick, trying to elicit some pain until there are grating noises and she's using a lot of force. I try to brace myself against the inevitable scream, the reaction I will surely have as I reflexively leap out of the chair once the pick stabs into soft tissue. Mercifully, it doesn't come. Absurdly, I realise halfway through the pick ordeal that the dentist is also risking her well-being by putting fingers in my mouth. At any moment I could shut my teeth and bite. This actually gives me a semblance of control over the situation and I am able to hang onto this through my fear. She spreads a generous amount of pina colada-flavoured numbing gel in my mouth, and gives me three injections of anaesthetic. I don't think my British dentist did this to me the last time I had fillings, so I mentally chalk one in favour of Amsterdam dentistry. Of course, he might have just been saving me money. Since 2011, dentists here have been permitted to raise the prices of their treatments above fixed rates, and they have done so despite a slew of grumbling complaints from the Dutch public. I spend the whole session staring fixedly at a black blob in the fluorescent light, drawing out the debate in my head about whether it is a spider or not. The actual drilling and filling does not take long, but after the resin has been packed in, there is about 20 minutes of reshaping and grinding down the resin so that it fits into place neatly when I put my teeth together. I decide that it is a spider, and it's dead now. Afterwards I have to go and pay. It's rather more than I expected. The anaesthetic has spread its rubbery coldness up my cheek and into my nose, which stings and runs all day. Dr. Tsang wanders in and out of the reception and treatment room, eating something crunchy as he does. At least he did not do this while my mouth was splayed open. I ask him once more about how much braces would cost. "How much is it in England?" he asks first. I don't remember, other than it being enough to put me off getting them. "I could probably do them for about 2000 euros," he finally says, still supremely uninterested. I've never met a less interested dentist. I feel our interaction has been exhausted. I am beaten. At that point, a man lurches into reception. He has a homeless look about him, a thousand-yard stare with eyelids ratcheted obligingly back and out of the way of his stare. He wordlessly bares a set of separated, yellow teeth at us, pointing at his lower gums. "Yes, can I help?" Dr. T says mildly to this silent, staring, mouth gaping man. He is certainly unflappable. They stare at each other. I turn to punch in my code into the PIN machine and pray that my health insurance will sort out the costs quickly. Thankfully, when I turn around again, the strange man has left and I have a clear route to the door. Amsterdam Dental. No, I would not recommend them. |
AuthorNot quite a blog, but things that I have written. Please note - these writings are unedited, for the purposes of flexing my fingers, and no doubt contain grammatical errors and carelessness of expression I wouldn't allow in professional writing. Categories
All
Archives
June 2021
|




















 RSS Feed
RSS Feed

{kind=link}