|
Picture yourself on a mountaintop. The piercing cold temperature. The unbarred views. The thin air.
Dr Hugh Montgomery presented the mountaintop to us as a natural laboratory space. As Director of UCL Institute for Human Health and Performance, and Professor of Intensive Care Medicine, Hugh is interested in how the human body responds to exercise. And the mountaintop presents an extreme environment for a particularly elite class of exercisers, the mountaineers. Not only is mountain climbing a gruelling challenge for the body's muscles, but climbers must also tolerate low levels of oxygen in the air. The higher they climb, the lower the oxygen levels fall. But by studying the physical changes that mountain climbers undergo on a climb, and scrutinising the underlying genetic causes, Hugh's research group have produced some startling lessons for critical care of hospital patients. Hugh, smiling and fresh-faced, took to the stand at Bristol M-Shed to discuss his research. He is the kind of researcher who deserves his own HBO television show. This hypothetical show would incorporate genuine scientific research, as well as offering plenty of scope for macho posturing and man vs. death escapades on the mountaintop. Indeed, the man's achievements and hobbies would make any fiction unnecessary. A diver, a record-breaking underwater piano player, an 'occasional' ultra-runner, a mountaineer, author, screenwriter, and a pioneering cardiovascular geneticist. I could easily add more, but I am already lost in awe. "Studying acute physiology can tell you really important things about yourself, and patients," said Hugh. He began by outlining the key scientific tools that we needed to understand. Angiotensin is an important hormone for your blood system, and the renin-angiotensin system (RAS) controls the blood pressure of the body. It is a network of different hormones, including angiotensin, which tweak the size of blood vessels and the amount of water kept in the blood. A key controlling element is angiotensin-converting-enzyme (ACE). A high level of ACE in your RAS raises your blood pressure. "That's where it stopped when I was in medical school," said Hugh. "But it turns out, like most things I was taught at medical school, that wasn't half the story. Because these systems are everywhere - in plants, in locusts, in fish, in jellyfish- all things that have been there for millions of years. And jellyfish don't even have blood pressure!" So RAS and ACE must affect more than blood pressure. In fact, they are found in a huge range of human bodily tissues, from your brain to your eyeballs to your skin. It is now understood that ACE also influences cell growth, inflammation, and metabolism in body tissues, even if the finer details of how it does this are still being uncovered. In the 1980s, it was observed that increased amounts of ACE in rats leads them to develop bigger hearts. Knockout the ACE gene, and hearts can't grow in size. In humans, the old romantic maxim is untrue. Having a big heart is not a good thing - unless your heart has become big due to regular exercise. Otherwise, a large heart is associated with a higher likelihood of heart attack. So whatever causes the increase in size also damages the heart tissues. Based on the studies of ACE and heart size in animals, Hugh needed to see if the link between ACE levels and heart size applied in humans. His group had found two different ACE gene variants - the I allele, and the D allele. People with the I allele produced lower amounts of ACE. People with the D allele produced more ACE. And because everyone has two copies of each gene, any human could have II, ID, or DD. But based on rules of inheritance, in a group of people 25% will have II, 50% will have ID, and the final 25% will have DD. So if Hugh could take a group of humans, measure the differences in their heart size, and then correlate the heart size to the different genes, he would be able to prove ACE was affecting heart size in humans. But how could this be done, and more so, done ethically? There could be many confounding factors affecting heart size. Hugh found the perfect experimental subjects in the form of military recruits. Military recruits all undergo the same strict regime of training and diet. Exercise naturally causes heart growth. So at the end of 8 weeks of training, Hugh would be able to measure differences in heart size, and link this to the I or D alleles. After 8 weeks of training, the recruits with II alleles - producing the lowest levels of ACE - showed heart growth of approximately 2%. In DD recruits, who produced the highest levels of ACE, the heart growth was 6%. Hugh sketched out the scientific reason that ACE caused heart growth. In the RAS system, ACE breaks down kinins, proteins which are involved in blood vessel dilation. High ACE equals low levels of kinin, which means greater growth in heart size. As in most science, the chain of cause and effect was becoming a little long, but we were still with him. So the military recruits proved the link between ACE and heart size. And there was more. Through a muscle fatigue test- a fancy way of saying, how long could each recruit hold a weight at arm's length without buckling - it was proved that II recruits have the best response to exercise. ID recruits respond moderately to exercise, showing only small improvement in muscle fatigue after training. DD, statistically speaking, showed no better improvement by end of their training. Now, back to the mountains. Mountain climbers with II are more likely to reach the peaks than DDs. Similar trends can be seen in other oxygen-hungry sports, like marathon running, where runners are much more likely to have II alleles. Hugh revealed another interesting tidbit. Although gruelling endurance challenges like the Tour de France are dogged by doping scandals, where athletes use erythropoietin hormone to increase red blood cell loads, the ability to accumulate more oxygen on a mountaintop is not actually helpful to your body. To put it more simply- if you put a Tibetan and a Westerner on a mountaintop, the Tibetan's body will generate less haemoglobin. The genetic selection for successful living at high altitudes appears to be in keeping haemoglobin lower. Hugh explained that I or D alleles affect how efficiently mitochondria use oxygen. Mitochondria are the power plants of the cell, generating ATP energy from oxygen. Low ACE levels make mitochondria better at generating ATP from oxygen, even low levels of oxygen. D alleles are more like "leaky batteries" - they lead to a higher level of ACE in the body, which raises oxygen demand. "So what genetics is telling us, is that when oxygen availability is low, we should try to increase the efficiency in which we use the oxygen," commented Hugh. He recalled that the convention treatments for ICU patients in hospital is to try, forcibly, to put oxygen into their bodies. But modern treatment needs to change, as studies have shown forcible oxygen transfusions can increase mortality. Based on lessons from mountaineers, new modes of treatment are being introduced into hospitals to allow oxygen levels to reach lower levels than conventional treatment had allowed. A normal person has an oxygen tension of 12 kPA. On a ward, lower levels of 8 kPa is now being allowed. A level of 6 kPA is still considered very worrisome. However one experienced mountaineer has been able to reach 2 kPA. This is conventionally considered terminal... but for him, it was not. His body was attuned to that low level of oxygen. Many animals adjust their body systems to withstand low oxygen environments. These include a few fish with coincidentally interesting names - the epaulettes shark, the oscar fish, and the Crucian carp - who shut off unnecessary body functions when oxygen levels decline. With a wry grin, Hugh admitted that when he explained his research to his 6-year old son, he was told his research was "very obvious". When a car is low on fuel, you don't leave all its systems running, you tune down to the bare essentials. Why had it taken his father 20 years to work out that the human body does the same? But the most startling and sobering impact of ACE was yet to come. Hugh showed us the relationship between the ACE gene variants and medical conditions, especially in the ICU. In premature babies with under-developed lungs, high ACE levels are associated with respiratory distress. In patients who undergo bypass surgery, II patients with low ACE show better survival rates. In meningitis patients, having the DD alleles is associated with the most severe examples of sudden meningococcal sepsis. It was sobering to realise that survival, especially in the face of respiratory complications, could be so clearly linked to the ACE gene. "In this audience, if we all came down with Adult Respiratory Distress Syndrome and ended up in Bristol ICU, the IIs could have a 90% chance of surviving. Whereas DDs have an over 55% chance of dying. That puts my job in perspective. We like to congratulate ourselves as how good we are when someone lives - but a lot of that living and dying, is down to our genes." Hugh moved onto another lesson of mountaineering - starvation. Hypoxia, meaning low levels of oxygen, causes weight loss. Mountaineers lose both fat and muscle in the hypoxic conditions of the mountain. ICU patients, whose body tissues are low in oxygen, also show weight loss. A key clue is that muscle is lost, along with fat, even in highly active and well-fed mountaineers. A group of Hugh's mountaineers who scaled Everest lost 9 kg each, on average. Hugh explained that the 90% of the body's energy goes into producing protein, to rebuild and renew the body. It used to be thought that in low oxygen conditions, the body's regulation was simply thrown into disarray, causing inevitable weight loss. But now it is shown that the body actually orchestrates sophisticated survival plans. It tries to conserve oxygen by shutting down demanding systems. Essentially, the body willingly creates a 'starvation' mode. In starvation, a process known as ketosis occurs where fat is broken down for energy, producing chemicals known as ketones. This is the fundamental concept of the Atkins diet. Ketosis is also carried out by hibernating animals. It appears likely that ketones have some kind of beneficial effect. And this is true. Ketones are an anticonvulsant, which is why the severity of epileptic fits can be reduced by putting patients on diets. Ketones protect the brain from hypoxia and low levels of glucose. Even sperm are more motile in ketones, and the heart increases its workload. In short, starvation can actually be beneficial. A synthetic ketone is being trialled in adults with heart failure in Belgium, and there are more studies which will test ketone compounds with patients and premature babies. And studies have shown that force-feeding of ICU patients in hospital can lead to muscle wasting, a new method of intermittent, low feeding may prove much more helpful. Perhaps a more modern and effective treatment needs to accept starvation as one of the body's natural defence mechanisms. There's some truth in granny's advice - 'feed a cold, starve a fever'. Ketones, ACE, genes, and fitness. I wondered what would my genotype be. Did I respond to exercise well, like an II, or fall in between, as an ID? I have only ever ventured up a bouldering slope, but I have dreams of climbing Kilimanjaro. How much extra preparation would I need? "Should I take ACE inhibitors to improve my chances of reaching the summit of Everest?" asked an audience member, a self-diagnosed DD. "Yes... but we haven't done the study yet." The study is in the planning stage, but they still don't know how ACE inhibitors will react with the body in hypoxic conditions. This is too big a risk to take on a mountaintop. And throughout his talk, Hugh pointed out that D alleles were not to be perceived as inferior. This is the first gene that was discovered which was directly related to fitness. It has some striking lessons for hospital care. But it is not a case of genetic determinism, stating who is likely to be the best at keeping fit, or surviving overall. The D allele confers its own benefits. People with DD appear to be more resilient to haemorrhage. And they are likely to be stronger, better at swimming and sprinting. They tend to show greater muscle mass in old age which significantly reduces the problems of frailty and falls. I thought of my father, silver-haired and 70-something, still stomping round, still operating heavy machinery, still involved in the mysterious and never-ending movings of heavy objects around his property. For that matter, I also thought of my mother, thin, frail, and disabled, but who has been doggedly picking up an entire bulldozed bungalow, brick by brick, and assembling them into an array of neat stacked cubes in her garden (don't ask). I might never know my genotype for I or D and I might find it hard to predict, but it probably didn't matter anyway for my fitness. What matters is the mind - willpower, determination. For his part, Hugh was vehemently opposed to casual genotyping for these alleles. The research needed to carry on, and it would be too easy for, say, medical insurance companies to jump the gun and draw broad - and expensive - conclusions. After all, for all his incredible-sounding athleticism, Hugh himself is a DD. You can listen to a recording of Hugh's talk here ... And the following questions here ... Hugh Montgomery also talks about his discovery of the first gene for fitness to Jim Al-Khalili, on the BBC's The Life Scientific
0 Comments
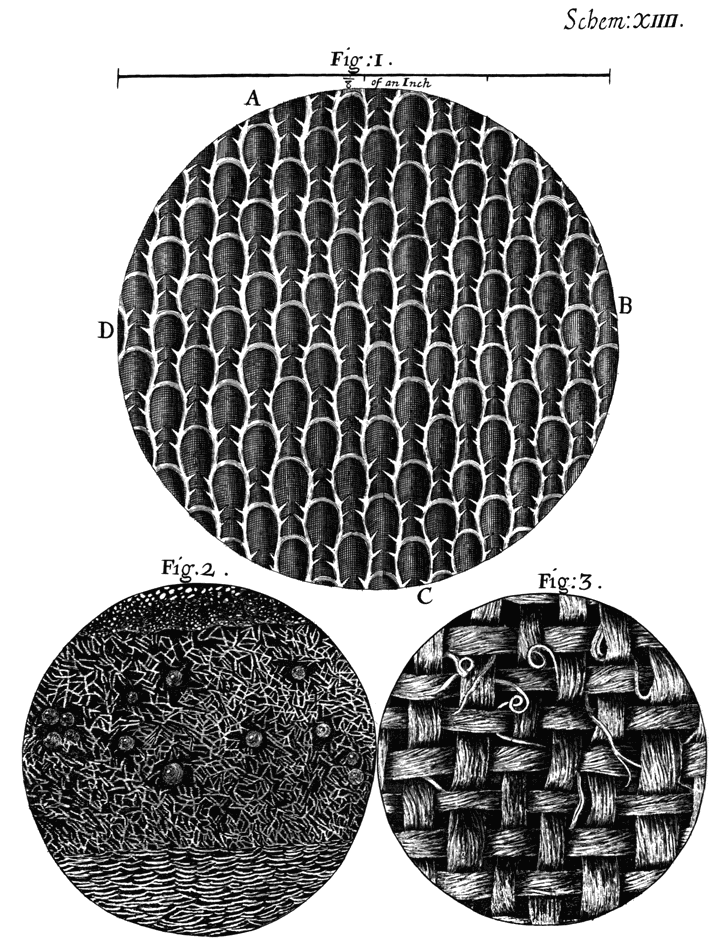
What is the romantic disease? Watch the film below to see artist Anna Dumitriu talking about her exhibition. 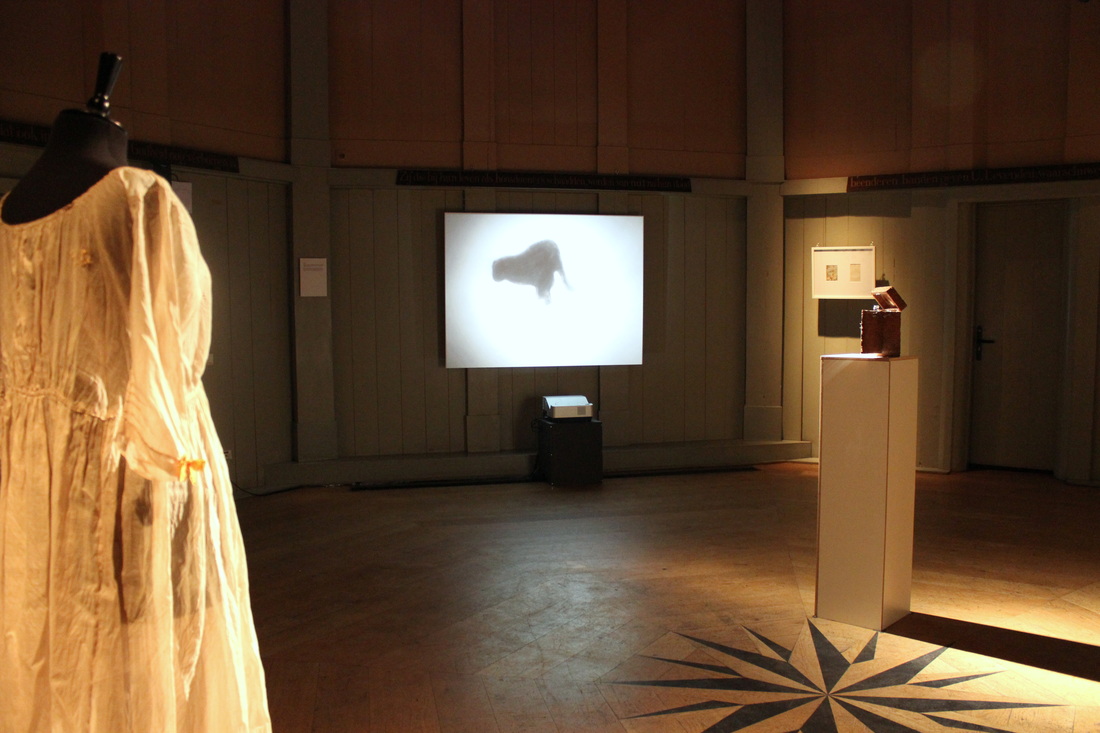 Anna Dumitriu explains the stories behind her exhibition here I’m in a room with humanity's biggest killer. It began eating away at us over 9000 years ago, and has never really stopped. The marks of our relationship surround me in an array of medical leaflets and dyed fabrics. Mysterious objects sit on stands. A glistening set of metal needles and devices inside a spongy wooden case. There's a tiny, bare bed, and a ghostly pale dress. A collection of tiny felted grey lungs that resemble a group of settled moths on a wall. This is an exhibition on tuberculosis. 'The Romantic Disease' has been created by Anna Dumitriu, a British artist with a taste for microbiology and emerging technologies. She is the artist-in-residence for the Modernising Medical Microbiology project, a collaboration between Oxford University and Public Health England, and she was inspired to create this exhibition by their research into bacterial diseases. The exhibition is on tour through Europe, and is currently hosted in the Theatrum Anatomicum at Waag Society in Amsterdam.  What caused tuberculosis? On one side of the room I see an animated black dog circling and pacing endlessly. It represents one early interpretation, the 'demon dog'. This dog would enter the bodies of sufferers and bark, making them cough. Later, people thought tuberculosis could be inherited. On another wall I read an old medical text warning of the 'tubercular taint' that could be passed on through risky marriage. I find out that the pale dress hanging on its stand is a Romantic era maternity dress, representing how some pregnant women with tuberculosis were forced to have abortions. It was a long time before the real cause was found. Bacteria were only seen for the first time in 1676 by Anton van Leeuwenhoek, and in 1882 the microbiologist Robert Koch proved that tuberculosis was caused by bacteria. 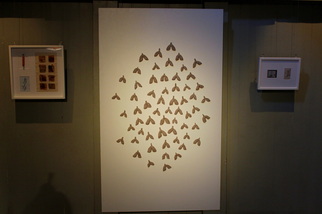 At the entrance to the exhibition I spy a quote from the Romantic poet, Lord Byron. ' “How pale I look! – I should like, I think, to die of a consumption –because then the women would all say, 'see that poor Byron- how interesting he looks in dying!” ' Ah, the vanity of poets. I wonder how tuberculosis could ever be thought of as 'romantic'. The disease was called 'consumption' from the 14th century because of its vampire-like effect on sufferers. It mainly eats away at the lungs, causing hacking coughs and bloody sputum, sweaty fever, the body weakening and wasting away. The statistics for tuberculosis are shocking. One third of the world's population are infected with Mycobacterium tuberculosis, the bacterium responsible for causing the disease. Of those, ten percent will develop the disease. Of those, around five percent would die of it without treatment. It is currently the second most deadly infectious disease after HIV and has killed far more people overall. While it is curable with modern antibiotics, in the right conditions extremely drug-resistant tuberculosis can evolve. So what's romantic about all of this? But I'm looking at this wrong. Nowadays, we know about tuberculosis. We know about bacteria. We have antibiotics and medical advice. We have scientists with gene sequencers and electron microscopes. But for most of our history, people did not know what caused, spread, or cured tuberculosis. Forced to live alongside this mysterious and widespread disease, unpicking its mystery with slow science, people also responded with myth, imagination, and art. After all, anyone could get tuberculosis, from famous figures to the unknown. Many Romantic Era artists like Keats had it. Perhaps Byron spoke tongue-in-cheek, since his own father died of the disease. And unlike other common diseases of the time, like smallpox, tuberculosis was less devastating on the appearance. A waifish, pale appearance was even considered fashionable, tuberculosis or not. This is not so different from today's unchanging fashions of the catwalk, or tastes for sparkly skinny vampires, then.  And while many artists had tuberculosis, could tuberculosis actually create the artist? Some people have theorised that tuberculosis enhanced creativity by inducing spes phthisica, a state of euphoric creativity before death. While it's likely that this state was only based on romantic anecdotes, perhaps a feverish delirium could inspire strange and artistic ideas. Anna showed me around the exhibition, inside the softly lit circular room of the Theatrum Anatomicum. Her artworks tell the story of how we have long tried to understand tuberculosis. “Because it's had such an impact on humanity, there are a lot of myths around tuberculosis,” Anna says. “And there's a lot of different areas of medical research that have changed over time. There's this fascinating cultural story alongside the microbiological side.”  How was it transmitted? “Where there's dust there's danger,” warns a 1902 guide by the National Society for the Prevention of Consumption. At this time, tuberculosis was thought to be spread mainly by infected spit that dried on specks of dust. Invite a few tuberculosis sufferers into your home, let them spit on the floor, neglect to sweep for a few weeks, and eventually you could be stirring up clouds of death with your broom. Close up, I see the moth-like objects on the wall are actually tiny grey lungs. These are made from felt and dust, by Anna and people who have attended her interactive workshops. The advice was almost right in that tuberculosis can be spread by sputum, sprayed into the air by coughing, but dust could not spread tuberculosis. Drying out sputum droplets tends to kill the bacterium.  Today, thanks to whole genome sequencing, transmission of a disease can be more precisely mapped. I learn about this by examining a stand holding an old 'pocket-bottle for coughers'. The Blue Henry is an attractive blue glass bottle with a silver lid, intended to provide a safe and fashionable receptacle for sufferers to cough up blood in public. Like many of the artworks on display here, Anna has combined the past and present of tuberculosis on this object. The top is engraved with a patient transmission map, produced by the research of the Modernising Medical Microbiology (MMM) project. Today, the MMM scientists investigate deadly bacterial diseases by sequencing the genomes of the bacteria responsible. Using the sequences, they can identify which strains are responsible for disease outbreaks, and they can also map the transmission of an outbreak back to its source. The diagram on the lid of the Blue Henry shows how multiple people were infected by one person, who was in turn infected by Patient Zero, the first person to get the disease. Prior to whole-genome sequencing, unravelling the spread of a disease would have relied on a laborious process of interviews and piecing together likely infection scenarios. How was tuberculosis treated? There are fascinating items showing how tuberculosis treatments were marketed. 'REST... to beat TB' one medical poster declares, showing an improbably merry man as he lies in bed, resting off his tuberculosis. Resting was supposed to help recovery by lowering the breathing rate and giving the lungs of sufferers less work to do. Patients would also be shuttled off to sanatoriums in mountainous regions, where the air was thinner and thought to be better for the body. Anna tells me about an infamous Welsh mountain sanatorium, Craig-y-nos, where children were forced to sleep outside in fresh yet painfully frosty air, since this was thought to be another benefit. A jaunty magazine poses an attractive young couple under the headline, 'I had TB!'. Below this, Anna has arranged an innocuous little microscope slide of stained M. tuberculosis from sputum, the foe in question.  But there are also works based on more sinister tools. Anna explains that artificial pneumothorax- collapsing a lung- was once a common treatment. The idea was that collapsing the lung would 'rest' it, giving the lung a break to tackle its tuberculosis infection, and also starving the tuberculosis bacteria of oxygen. Around one third of tuberculosis patients were treated to this between the 1930s to 1950s, including the writer George Orwell. It's a toe-curlingly unpleasant idea, but Anna tells me that some small, recent trials suggest this antiquated treatment might help fight the modern rise of extremely-drug resistant tuberculosis. Sometimes medicine, like history, turns in cycles.  Textiles and dyes also play a large part in the history of tuberculosis. The maternity dress has been dyed with walnut husks, madder root and safflower. All common natural dyes, and all early treatments for tuberculosis. There's a vial and fabric-stains of Prontosil, the world's first 'sulfonamide' drug which could slow the growth of bacteria. It was produced by Bayer, today known as a chemical pharmaceutical giant, but who began as a dye manufacturer. Bayer's large chemical laboratories for producing dyes were perfect playgrounds to test out new chemical combinations. With ready supplies of coal tar, a by-product of coal production, a base for many dyes, and the bane of my childhood thanks to my dad's inexplicable fondness for coal-tar soap, many scientists tried to produce dyes to specifically target bacteria. Along with other useful products like aspirin, Bayer eventually produced Prontosil, and medicines derived from this bright red substance were widely used in bandages during WWII. It also had the side effect of dyeing the skin red. Anna has also found staining effects in modern treatments for tuberculosis, and she used the growth media for Bacillus Calmette-Guerin (BCG) (an attenuated strain of Mycobacterium bovis used as a vaccine for TB) to add striking touches of pale blue to some of her artworks.  I also find out that Byron's vain wish to be pale and interesting would get a colourful update. Anna reveals that a modern antibiotic used to treat tuberculosis, rifampicin, can cause the tears and sweat to turn orange. “In a way, they look like they have a nice tan,” she commented wryly. “So it's interesting how that link between fashion, appearances and tuberculosis has come about again.” Stories and the Sublime Anna is fascinated by objects that are tainted with the story of the disease, and has added more subtle combinations of old and new stories. The dress and tiny lungs are infused with the extracted DNA of M. tuberculosis. There is no danger that the DNA can harm anybody. But the DNA's presence in objects so close to me make me feel face-to-face with the bacterium itself, laid open before me. It is an intimate and respectful meeting, one without infection, disease, or pain. “My research into this exhibition began with conversations with scientists, and reading about the disease, and the more I did the more stories I found. The strangeness of everything, the stories, it's not really what people expect,” reflected Anna. “I'm definitely planning to take the work further, I think there's many more stories to be told.” She also runs hands-on workshops to explore the history of tuberculosis further, and sometimes people attend who have experienced old tuberculosis treatments first-hand.  Looking round the exhibition, I'm struck by how much it has filled in the cultural side of tuberculosis to me, something which was entirely missing when I studied the disease at university. In modern times we might easily think that only the scientific view remains now. With sophisticated technologies or new drugs, scientists work towards understanding cause, transmission, and treatment in ever closer detail. But cultural understanding of the disease is something uniquely human. And inspiration and appreciation of the microbiological world play a vital role in pushing scientific discoveries. Anna points out that microbiology is still a relatively new science. It was only a few hundred years ago that Anton van Leeuwenhoek, a textiles dealer, first saw microbes under his homemade microscopes. Van Leeuwenhoek was not a scientist, he was a textiles dealer used to examining thread counts under magnifying glasses. Yet he was inspired to explore the microscopic world after seeing pictures from Robert Hooke's 1665 book, Micrographia, with its detailed illustrations of textiles in the microscopic world. Van Leeuwenhoek went on to make a number of groundbreaking discoveries in science, and was always guided by his interest and appreciation in what he saw. “We're at a fascinating time when new technology is available and revealing more about the microbial world,” Anna said. She is also looking forward to exploring our relationship with other infamous bacteria, including artworks based on Staphylococcus aureus, the agent responsible for MRSA.  I asked Anna what she wanted people to go away from the exhibition with a sense of. “To me bacteria have this effect of the sublime. With all the effect they've had on humanity, but the fact that they're fascinating and beautiful too. Ideally I'd like people to come away from the exhibition with a sense of the bacterial sublime, to understand the sea of bacteria they're a part of, and that they're super-organisms containing bacteria. I'd like people to understand that.”  Additional Information
Anna Dumitriu explains more about her artwork and inspiration in this film. Anna Dumitriu received a Leverhulme Trust Artist in Residence Award in 2011 to work with the Modernising Medical Microbiology project led by the University of Oxford, Nuffield Centre for Clinical Medicine, in conjunction with Public Health England. 'The Romantic Disease' exhibition is funded by the Wellcome Trust. The exhibition will be shown at the Waag Society until 27th July, and the Art Laboratory in Berlin from 26th September - November 2014. Links Anna Dumitriu's website: http://normalflora.co.uk/ Modernising Medical Microbiology website: http://modmedmicro.nsms.ox.ac.uk/ Waag Society: http://waag.org/en/event/romantic-disease-exhibition Further reading
|
AuthorNot quite a blog, but things that I have written. Please note - these writings are unedited, for the purposes of flexing my fingers, and no doubt contain grammatical errors and carelessness of expression I wouldn't allow in professional writing. Categories
All
Archives
June 2021
|
 RSS Feed
RSS Feed

{kind=link}